Puberty Blockers: An unregulated live experiment on children
by Gráinne Mhaol
17 April 2021
...it felt as if we were part of something that people would look back on in the future, and ask, what were we thinking? Former Tavistock Clinician (1)I have previously covered a few issues which I think should be borne in mind when looking at medical interventions in this area. These were primarily to do with medical safeguarding and the vulnerabilities of gender non-conforming patients being seen at gender clinics for young people. These can be read here:
A new front in human liberation,
or a medical scandal in the making?
http://www.socialistdemocracy.org/RecentArticles/RecentANewFrontInHumanLiberationOrAMedicalScandalInTheMaking.html
And
Vulnerable children being
seen at Gender Clinics
http://www.socialistdemocracy.org/RecentArticles/RecentVulnerableChildrenBeingSeenAtGenderClinics.html
It should also be borne in mind that sexism and homophobia seem to be largely behind non-conforming children being labelled as different, born in the wrong body, and in need of medical intervention. (2,3) As one clinician in Britain commented Childrens bodies are being damaged in order to treat societal issues (4).
In this article I will talk about the diagnosis of gender dysphoria in children and the potential complications of medical interventions. I am not a medical professional but will do my best to present evidence which shows that there are some serious concerns over medicalising gender non-conforming children. I think the evidence speaks for itself.
Sexism in Diagnoses
Looking at the HSE website, the diagnostic criteria for gender dysphoria is based to a large extent on children engaging in gender-non-conforming behaviour. So sexist adult expectations are driving the medicalisation of gender non-conforming children.
This is from the HSE website on Signs of Gender Dysphoria [Ive emphasised a few parts in bold]
People with gender dysphoria...may feel so unhappy about conforming to societal expectations that they live according to their anatomical sex, rather than the gender they feel themselves to be.
Gender dysphoria behaviours
in children can include:
insisting they're of
the opposite sex
disliking or refusing
to wear clothes that are typically worn by their sex
wanting to wear clothes
typically worn by the opposite sex
disliking or refusing
to take part in activities and games that are typically associated with
their sex
wanting to take part
in activities and games typically associated with the opposite sex
preferring to play with
children of the opposite biological sex
disliking or refusing to
pass urine as other members of their biological sex usually do
insisting or hoping their
genitals will change
feeling extreme distress
at the physical changes of puberty
The HSE website does acknowledge: Children with gender dysphoria may display some, or all, of these behaviours. Behaviours such as these can be part of childhood and don't necessarily mean your child has gender dysphoria. (5)
But the HSE don't explain why behaviours can be interpreted as both normal, and evidence of a clinical problem.
The section on diagnosis is worrying. This is what the HSE website has on diagnosis in children (the emphasis on clothes is particularly worrying):
Criteria for children
To be diagnosed with gender dysphoria, a child should experience the following for at least 6 months:
1. Want to be the same
sex
Repeatedly insist they want
to be the opposite sex, or they are the opposite sex, and behave as the
opposite sex. This must not be just because they want the supposed advantages
of being the opposite sex.
2. Dislike of certain
clothes
Dislike or refuse to wear
clothes typically worn by their sex and insist on wearing clothes typically
worn by the opposite sex. Or show dislike or unhappiness with their genitalia
and insist that it will change into that of the opposite sex. For example,
refusing to pass urine as members of their sex usually do.
3. Puberty
Have not yet reached puberty.
Misleading Claims by The HSE
In the Gender Dysphoria section of its website, the HSE astonishingly claim that it is possible to change ones sex via surgery. This is claimed five times in this section, for example, stating: Some transgender people seek to have surgery to permanently alter their biological sex (5)
The HSE website also talks about surgery to create a functioning vagina or penis. This suggests a fundamental misunderstanding of both human anatomy and the surgery. From the HSE website:
A phalloplasty uses the existing vaginal tissue and skin taken from the inner forearm or lower abdominal wall to create a penis. A metoidioplasty involves creating a penis from the clitoris, which has been enlarged through hormone therapy.
The aim of this type of surgery is to create a functioning penis (5)And
The surgery aims to create a functioning vagina with an acceptable appearance and retained sexual sensation.(5) [my emphasis in bold]This section of the HSE website makes no reference to the high risk of complications, nor to the poor outcomes of these surgeries. I will give some examples of poor outcomes in a future article.
It is no wonder children can be confused about these issues when the HSE puts such misleading information on its website.
Medical Interventions

Gender critical women at
Auckland Pride. More info https://reneejg.net/2018/02/feminist-pride-action-support/
The main medical intervention aimed at children in Ireland is the prescription of puberty blockers. Once children reach the age of 16, they can be put on cross-sex hormones. It looks like surgery wont be carried out in Ireland until the patients are at least 18 years of age. As far as I can ascertain, patients here are currently referred abroad for surgery via the Treatment Abroad Scheme (6). I assume only adults are referred
In countries such as the US, some surgeries, such as double mastectomies, can be carried out on girls as young as 13. If safeguarding is removed, and a so-called informed consent/affirmation only model, is introduced in Ireland (as discussed earlier http://www.socialistdemocracy.org/RecentArticles/RecentANewFrontInHumanLiberationOrAMedicalScandalInTheMaking.html ) then we could see more invasive interventions allowed on children here too.
Until recently children in Ireland were referred to the London based Tavistock & Portman Gender Identity Development Service (GIDS). A clinician came to Ireland once a month to see children here, and patients were apparently seen via video-link during part of the pandemic (7). The Tavistock was responsible for training Irish clinicians in diagnosis and management of Gender Dysphoria in children (8). The British-based Gender Identity Development Service (GIDS) will no longer be seeing Irish patients and the HSE is planning to set up a service here, but GIDS will already have been very influential in terms of the approach taken.
I think the two most significant pieces of information regarding children who are gender dysphoric are as follows:
(a) As Dr Margaret McCartney wrote in the British Medical Journal No blood test or brain scan can tell which person with gender dysphoria will do better or worse with the medical and irreversible surgical treatments on offer.. (9) There also seems to be no clinical method that can establish this either. As a GIDS clinical psychologist, Dr Aidan Kelly, said: Often we are putting responsibility back on the family because we dont have the evidence base to say its these kids and not these kids or how we can pick out which kids should go forward and which kids shouldnt(10)
b) Most children do not persist in wanting to be the opposite sex beyond puberty. It doesnt make sense to medicate them out of a potential cure. Because of this, one study suggested:
As children with GID [Gender Identity Disorder] only rarely go on to have permanent transsexualism, irreversible physical interventions are clearly not indicated until after the individual's psychosexual development is... complete. The identity-creating experiences of this phase of development should not be restricted by the use of LHRH analogues that prevent puberty. (11) [my emphasis in bold]A study just published in March 2021 reported: This study reports follow-up data on the largest sample to date of boys clinic-referred for gender dysphoria...Of the 139 participants, 17 (12.2%) were classified as persisters and the remaining 122 (87.8%) were classified as desisters. This means only 12.2% still had significant gender dysphoria on follow-up, a fraction of those initially referred. (12)
Another paper that looked at ten different studies reported that The conclusion from these studies is that childhood GD [Gender Dysphoria] is strongly associated with a lesbian, gay, or bisexual outcome and that for the majority of the children (85.2%; 270 out of 317) the gender dysphoric feelings remitted around or after puberty. (13)
Even the HSE website recognises this and says on its website:
The Endocrine Society found that 75-80% of children who were diagnosed with gender dysphoria before they reached puberty did not have the condition after puberty. Therefore, endocrine treatment is not recommended until after puberty, when a diagnosis of gender dysphoria can be confirmed. (14)For some reason, in spite of knowing this, Irish children can still be put on puberty blockers.
First Do No Harm
If a first do no harm approach were to be adopted in the management of children with gender dysphoria it is hard to see that any child would be put on puberty blockers, on the balance of probabilities of it doing more harm than good.
There is a practice in medicine called watchful waiting. This is the approach taken when there is uncertainty about the diagnosis, uncertainty about the best course of action, or when the risks of an intervention outweigh the potential benefits. Some people suggest this type of approach is best in the case of gender dysphoric children, with supportive counselling to help them get through puberty, and then reassessing options after that.
Puberty Blockers
Given paucity of evidence, the off-label use of drugs in gender dysphoria treatment largely means an unregulated live experiment on children. Carl Heneghan, director of the Centre of Evidence-based Medicine, University of Oxford (15)Puberty blockers are generally the first drug children diagnosed with gender dysphoria will be prescribed, if they are prescribed medication (not all children with gender dysphoria will be medicated). These medications are also known as chemical castration, and have been used for: men with prostate cancer; children with very early puberty (e.g. 7 years of age or younger in girls) to delay it until they are older; as a short-term treatment for some gynaecological issues in women; and on sex offenders. Interestingly, a paper reviewing the use of these drugs on sex offenders recommended that they should be reserved for patients with a paraphilic disorder and the highest risk of sexual offending because of their extensive side effects(16)
The reason puberty blockers are used in children who are gender dysphoric is that they halt the development of secondary sex characteristics, such as breasts in girls, or a deeper voice or facial hair in boys, which can cause distress. Another reason is that boys who go through natural puberty will pass less easily as women in later life if they have developed a deep masculine voice, a beard, a more prominent adams apple, or a typically male height.
Depending on what stage of puberty blockers are given, and if the child/young person goes straight on to cross-sex hormones without going through natural puberty, the young person may be made permanently sterile, as well as risking future sexual dysfunction (including a lack of sex-drive and inability to orgasm) and other possible negative health effects. (17, 18)
Im trying to avoid being too graphic in this piece, but one thing that needs to be mentioned is that if boys go on puberty blockers very early, and then proceed to cross-sex hormones without going through puberty, their penises will not develop normally and they will not have enough penile tissue for a vaginoplasty, even if they want to go through with genital surgery to create a pseudo vagina when they are older. In cases like this, tissue has to be removed from elsewhere, for example the colon, and the results can be very poor (e.g. there have been reports of genital areas smelling of faeces, even years after surgery, along with other post-surgical complications).
One known side-effect of puberty blockers is a negative effect on bone health. In children given puberty blockers for precocious puberty, some develop early osteopenia or osteoporosis. They are used in precocious puberty to delay puberty until they child is a bit older, not stop it for life.
This is one example of a case of a woman given puberty blockers for precocious puberty:
For years, Sharissa Derricott, 30, had no idea why her body seemed to be failing. At 21, a surgeon replaced her deteriorated jaw joint. Shes been diagnosed with degenerative disc disease and fibromyalgia, a chronic pain condition. Her teeth are shedding enamel and cracking.
None of it made sense to her until she discovered a community of women online who describe similar symptoms and have one thing in common: All had taken a drug called Lupron.
...It just feels like Im being punished for basically being experimented on when I was a child, said Derricott, of Lawton, Okla. Id hate for a child to be put on Lupron, get to my age and go through the things I have been through. (19)The same article quotes a parent who had a child who had been prescribed Lupron
'As a parent, I kick myself, says Jeanne Walsh, a Temecula, Calif...Walshs daughter took Lupron for precocious puberty and now struggles with fibromyalgia and has had jaw-joint surgery. What was I thinking?' (19)
Puberty blockers may also
have a negative effect on mood, IQ and mental development.
There have been lawsuits
against the manufacturer of Lupron, the maker of one type of puberty/hormone
blocker. (20) This website also lists some of the potential problems with
Lupron https://www.hormonesmatter.com/they-say-lupron-safe/
Are Puberty Blockers a Pause to Allow Time for Reflection?
Even though puberty blockers have been described as a pause to give children a chance to think through whether they want to continue on the path to cross-sex hormones and potentially surgery, in practice almost all children who are put on puberty blockers will go on to take cross sex hormones. (21,22, 23) Part of the problem with thinking that puberty blockers give children time to think about their options is that the blockers may keep the children in a pre-pubescent mental state to some extent, and the children do not get to go through the physical and emotional changes of puberty which seem to lead most to re-identifying with their birth-sex.
So looking at the information
available to us, the choices seems to be:
(a) Allowing children with
gender dysphoria to go through natural puberty and supporting them through
the stress of it, knowing the desire to be the opposite sex will fade away
for most.
Or
(b) starting a child on
potentially damaging medications and putting them on a medical pathway
for life (most of whom could have avoided it).
I think if a first do no harm approach is adopted, children would not be given these drugs for gender dysphoria.
Extending Childhood
One thing I have noticed is that puberty blockers are sometimes promoted by doctors as pausing the transition to adulthood. For children who are afraid of going through puberty, or struggling with growing up, this could be a very attractive option. One US medic, Dr Spack, has said What were offering is to extend childhood in a sense (24)
A similar comment was made by Dr Polly Carmichael, GIDS Clinic Director, in a programme aimed at children and aired on CBBC (Childrens BBC), I am Leo The blocker is an injection that someone has every month which pauses the body and stops it from carrying on to grow up into a man or a woman. And the idea of the blocker is that... we can take away that worry about your body doing something that you dont want it to...(25)
This could be music to some childrens ears, if they are scared of growing up, or not coping with changes puberty brings. It is important to remember that many girls could be experiencing sexual harassment for the first time at puberty, or on a bigger scale than when they were younger, and they might latch on to anything offering them a potential escape from this.
Change in Advice on Puberty Blockers
Until recently, puberty blockers were promoted as fully reversible by Britain's Gender Identity Development Service (GIDS), who were also treating Irish children.
In an open letter to the GIDS director, a former clinician who had worked under the service, raised a concern about how these drugs were being described to children and their families
GIDS clinicians tell children and families that puberty blockers/hormone blocks are fully reversible but the reality is no one knows what the impacts are on childrens brains so how is it possible to make this claim?(26)In a talk given by Dr Kelly of GIDS to the Irish Independent Guardian Ad Litem Agency (which represents the voice and interests of children in court proceedings), puberty blockers were presented as physically reversible (27) In fairness to him, at least in that talk he mentioned that they were not a benign intervention. I am mentioning the context of the talk as it could indicate that some people are thinking that the courts might in future be involved in cases of treatment decisions regarding minors. Id worry that vulnerable children in foster care could be put on puberty blockers, or that the courts might get involved in cases of disputed treatment. (This has happened in other countries.)
In the documentary I am Leo, mentioned above, which was aimed at children and which won a 2015 BAFTA award in the Childrens Factual section, GIDS Clinic Director Polly Carmichael said:
The blocker is an injection that someone has every month... if you stop the injections, its like pressing a start button and the body just carries on developing as it would if you hadnt have taken the injection. (I am Leo, 2014) (28)But a comment by Polly Carmichael the following year, at a conference in 2015, shows that she could make more cautious claims when speaking to clinicians:
The blocker is said to be completely reversible, which is disingenuous because nothings completely reversible. It might be that the introduction of natal hormones [those you are born with] at puberty has an impact on the trajectory of gender dysphoria. (The Guardian, 12 September 2015.) (29)The NHS in Britain used to claim that these drugs were reversible. Until May 2020, its website said:
The effects of treatment with GnRH analogues are considered to be fully reversible, so treatment can usually be stopped at any time (...) (30)But last May (2020) this script on the NHS website was changed to:
Little is known about the long-term side effects of hormone or puberty blockers in children with gender dysphoria.Although GIDS advises this is a physically reversible treatment if stopped, it is not known what the psychological effects may be.
It's also not known whether hormone blockers affect the development of the teenage brain or children's bones. Side effects may also include hot flushes, fatigue and mood alterations.(31)
Although not perfect,
and somewhat contradictory, its an improvement on what was there previously.
The change in advice from the NHS on puberty blockers may have been prompted by critical media coverage and a few legal cases that were being taken against the Tavistock & Portman NHS Trust, which oversees the Gender Identity Development Service (32,33,34). Ill cover one of these cases in the next article.
Thankfully this change of advice in Britain has led to a commitment to change advice from the HSE.
But a document for GPs, Information for General Practitioners Working with Transgender People, claiming Puberty Blockers were reversible, was still up on the HSE website until at least the 28th March 2021, months after committing to no longer making this claim. Thankfully this document seems to have been taken down now by mid-April 2021. (35) It is, however, still on the TENI (Transgender Equality Network Ireland) website with the HSE logo on it. (36)
It claims that treatment with puberty blockers is reversible. This is an image from it:
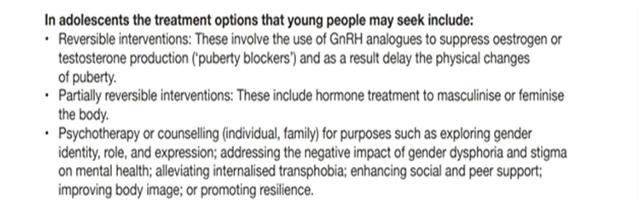
In February (2021) the Quality & Safety in Practice Committee of the Irish College of General Practitioners (ICGP), along with TENI, published its guidance, Guide for Providing Care for Transgender Patients in Primary Care Quick Reference Guide, which included the same claim that puberty blockers were reversible. That part seems to have been removed now, after the document got some negative public attention. But it is worrying that the HSE and the ICGP made this claim in the first place. An article here covers this issue in more depth https://womensspaceireland.ie/articles/the-icgp-and-teni/
NICE Review
The National Institute for Health and Care Excellence (NICE) in Britain published an evidence review in March (2021) looking at puberty blocker use in children with Gender Dysphoria. (37) Their assessment of the evidence was very critical. They pointed to the low quality of evidence for their use, and commented that there may not be any or much much change before and after treatment.
These are some quotes from NICEs reivew to give an idea of the problems they came across in assessing the evidence (some of the language is a bit technical. You can read a summary on the BBC website here https://www.bbc.com/news/health-56601386):
The studies included in this evidence review are all small, uncontrolled observational studies, which are subject to bias and confounding, and are of very low certaintyAll the included studies reported physical and mental health comorbidities and concomitant treatments very poorly
The results of the studies that reported impact on the critical outcomes of gender dysphoria and mental health (depression, anger and anxiety), and the important outcomes of body image and psychosocial impact (global and psychosocial functioning) in children and adolescents with gender dysphoria are of very low certainty using modified GRADE. They suggest little change with GnRH analogues from baseline to follow-up
However, as the studies all lack reasonable controls not receiving GnRH analogues [puberty blockers], the natural history of the outcomes measured in the studies is not known and any positive changes could be a regression to meanOutcome for the first patient to be put on puberty blockers
There is a lack of long-term information on how people will fare if put on this medical pathway early in life. But it is worth looking at the case of the first gender dysphoric patient put on puberty blockers. (38) Credit to Michael Biggs (Oxford University) for highlighting to this case. (39)
A paper was published on this patient in 2011. The patient had first been medicated in the 1990's.
According to the paper, this person was happy enough that they had transitioned. (This doesn't mean they couldn't have come around to acceptance of their biological sex if they had been let go through natural puberty and supported through it.) But, they had some worrying issues to do with their transition. He is used in the article I am quoting below, but to clarify it is a woman who identifies as a man that they are talking about. Interestingly enough they are same-sex attracted (i.e. they fit a common profile of female transitioners, and would be seen as a lesbian or bisexual had they not transitioned):
He was able to have orgasms, but he could not have sexual intercourse...At age 29, he had a serious relationship with a woman, which lasted for 5 years. However, he chose not to live together when the opportunity to do so arose. After his choice to continue living apart, his girlfriend ended the relationship, a few months before his interview at the clinic. This made him very much regret his lack of commitment. B considered it likely that his need to distance himself from her had been related to his shame about his genital appearance and his feelings of inadequacy in sexual matters...It seems, therefore, that B functioned well in most aspects of life, but that he was still struggling with the question, how to handle the dissatisfaction and shame about his genital appearance. (38)So to summarise some of the issues I've touched on in this and previous articles:
The diagnosis of gender dysphoria and labelling of a child as transgender, is driven by sexism sexism and homophobia.
Some health authorities have published information about the treatment for Gender Dysphoria that was/is misleading, and which is not backed up by evidence.
Some clinicians have given assurances about reversibility of puberty blockers to patients and their families which cannot be substantiated with evidence.
Clinicians have no objective way of knowing who might benefit from medical intervention and who will not.
The treatment, which is experimental, and potentially health damaging, can put a child with a healthy body on a medical pathway for life.
Most childhood dysphoria will resolve if/when children go through natural puberty, so treatment with puberty blockers and cross-sex hormones is like an anti-cure for many.
Some children and young people will end up sterile as a result of the treatment, and some of them will suffer sexual dysfunction as a result.
Given the evidence, it is hard to believe that puberty blockers continue to be prescribed to children. Part of the problem may be that its difficult for institutions to change course once a certain position has been adopted. This is partly because people who fundamentally disagree with the approach tend to leave that place of work, and people who agree with the approach stay and attract in others who think similarly, thus reinforcing institutional practices.
Sometimes the enormity of a mistake makes it more difficult to admit to and change course. As one former Tavistock clinician put it If they are getting it wrong, you have to ask, are they making kids infertile by mistake? Because if they are to truly acknowledge[our concerns], then they will have to ask themselves, what the f*** have we done to thousands of children? (40)
Thankfully some clinicians and former patients have been speaking up. I will discuss this in the next piece looking at the concerns about the Gender Development Identity Service in Britain and a Judicial Review of some of their practices.
Notes
(5) https://www.hse.ie/eng/health/az/g/gender-dysphoria/
(7) https://www.irishexaminer.com/opinion/columnists/arid-40188729.html
(8) Mentioned in this talk by a GIDS clinician. https://www.youtube.com/watch?v=kPlCGBBcw90
(9) https://www.bmj.com/content/360/bmj.k1312
(10) https://www.youtube.com/watch?v=kPlCGBBcw90
(11) https://pubmed.ncbi.nlm.nih.gov/19578420
(12) https://www.frontiersin.org/articles/10.3389/fpsyt.2021.632784
(13) Quoted in https://womensspaceireland.ie/articles/irish-children-and-the-tavistock/
(14) https://www.hse.ie/eng/health/az/g/gender-dysphoria/
(15) https://www.thetimes.co.uk/article/calls-to-end-transgender-experiment-on-children-k792rfj7d?t=ie
(16) Treatment of Paraphilic Disorders in Sexual Offenders or Men with a Risk of Sexual Offending with Luteinizing Hormone-Releasing Hormone Agonists: An updated systematic review Daniel Turner et. al 2018 https://pubmed.ncbi.nlm.nih.gov/29289377/ Mentioned by Michael Biggs in https://www.youtube.com/watch?v=9VHlkE40cFk&feature=youtu.be
(17) http://users.ox.ac.uk/~sfos0060/Biggs_ExperimentPubertyBlockers.pdf
(18) http://4thwavenow.com/tag/puberty-blockers-and-sexual-function/
(19) https://khn.org/news/women-fear-drug-they-used-to-halt-puberty-led-to-health-problems/
(20) https://www.lupronvictimshub.com/lawsuits.html
(21) No adolescent withdrew from puberty suppression, and all started cross-sex hormone treatment, the first step of actual gender reassignment.De Vires et al. https://pubmed.ncbi.nlm.nih.gov/20646177/
(22) After a median duration of 0.8 years (0.33.8) on GnRHa, 125 (87%) started gender- affirming hormones (GAH) [Note: by gender affirming they mean cross-sex hormones]... In conclusion, the vast majority who started GnRHa proceeded to GAH...Few individuals discontinued GnRHa, and only 3.5% no longer wished gender-affirming treatment. Brik et al https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7497424/
(23) At the end of the study one ceased GnRHa and 43 (98%) elected to start cross-sex hormones. https://www.medrxiv.org/content/10.1101/2020.12.01.20241653v1
(24) https://www.youtube.com/watch?v=kKMn4CymFTs&feature=youtu.be
(25) https://twitter.com/Newsround_Blog/status/1151821906707984385?s=20 You might need to scroll down to the clip from the BBC programme.
(27) https://www.youtube.com/watch?v=kPlCGBBcw90
(28) https://twitter.com/Newsround_Blog/status/1151821906707984385?s=20
(29) Cited by Michael Biggs in The Tavistocks Experiment with Puberty Blockers http://users.ox.ac.uk/~sfos0060/Biggs_ExperimentPubertyBlockers.pdf
(30) Archived page https://web.archive.org/web/20200502223746/https:/www.nhs.uk/conditions/gender-dysphoria/treatment/
(31) https://www.nhs.uk/conditions/gender-dysphoria/treatment/
(33) https://www.crowdjustice.com/case/gids-concerns/
(34) https://www.womenarehuman.com/safeguarding-concerns-raised-at-nhs-gender-clinic/
(37) https://www.evidence.nhs.uk/document?id=2334888&returnUrl=search%3ffrom%3d2020-01-01%26q%3dgender%2bdysphoria%26sp%3don%26to%3d2021-03-31 Direct link to download report here arms.nice.org.uk/resources/hub/1070905/attachment See also a BBC report https://www.bbc.com/news/health-56601386
(38) Cohen-Kettenis et al.2011 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3114100/ cited in The Tavistocks Experiment with Puberty Blockers* Michael Biggs Department of Sociology and St Cross College, University of Oxford (version 1.0.1, 29 July 2019) http://users.ox.ac.uk/~sfos0060/Biggs_ExperimentPubertyBlockers.pdf
(39) http://users.ox.ac.uk/~sfos0060/Biggs_ExperimentPubertyBlockers.pdf