Vulnerable children being seen at Gender Clinics
06 March 2021
We have left established evidence-based clinical practice and are using powerful life-altering medication for a vulnerable group of adolescents and children based upon a belief." Professor Christopher Gillberg, an expert in child and adolescent psychiatry, in a statement to a recent Judicial Review in Britain on giving children puberty blockers. (1)
A lot of young patients with gender dysphoria (extreme discomfort with their own sex), or who identify as the opposite sex, have multiple vulnerabilities. I am going to look at some of these below but first some background information to bear in mind.
Most children who have gender dysphoria, or a desire to be the opposite sex, do not persist in this desire by adulthood. This shows us that this is not a definite or fixed identity but can change over time. Clinicians have no definite way of knowing which children will persist in wanting to be the opposite sex/continue to suffer extreme discomfort with their own sex, and which won't. This is not even touching on the problems with medical interventions, which will be looked at in the next article.
One clinician from the British-based Gender Identity Development Service, who had been seeing Irish children referred there at the time, says this about the dilemma: often we are putting responsibility back on the family because we dont have the evidence base to say its these kids and not these kids or how we can pick out which kids should go forward and which kids shouldnt. (2)
One pattern that is emerging is that children who have vulnerabilities which might make them susceptible to bullying, or a more than average social pressure to conform, are much more likely to be labelled as transgender. It should be a red-flag to any clinician that there might be negative social influences at play in the development of the child's gender identity issues, and that it is not necessarily an expression of their true fixed self.
I'll explain now what some of the vulnerabilities are that these children have, and why I think this should give us some pause, before medicating these children, or affirming them (incorrectly) as really belonging to the opposite sex.
Homophobia driving transitioning
Ive gone into some detail
on the issue of homophobia driving some of the labelling children as transgender
in a previous article, so I won't repeat all of that here. This is a link
if you would like to read that piece:
http://www.socialistdemocracy.org/RecentArticles/RecentGenderIdentityIdeologyTransRightsMovementHomophobia.html
A few key point worth bearing in mind. Gender non-conforming behaviour in children and young people can give rise to homophobic reactions and attempts to normalise the child (in their eyes) by labelling them as the opposite sex. So a boy who likes dolls, dresses, and long hair gets labelled a girl rather than seen as a boy who like these things.
Same-sex attraction in teens can also lead to bullying which can sometimes cease or be reduced by identifying as the opposite sex, and there can be greater social support for some after coming out as transgender. [3]
Worryingly, some young people view being same-sex attracted as a confirmation of their identity as a person truly belonging to the opposite sex. One study found that all persisters [people who persisted in identifying as the opposite sex] reported feeling exclusively attracted to persons of the same natal [birth] sex, which confirmed their gender identity as they viewed this attraction as a heterosexual attraction. They did not consider themselves homosexual or lesbian. (4)
Recently, Dr Michael Bell,
Consultant Psychiatrist and former staff governor at the Tavistock Trust
(who run the Gender Identity Development Service), warned that transitioning
young people was a form of gay conversion therapy. You can see an interview
with him here:
https://www.youtube.com/watch?v=bHNh7lx2Z4U&t=2s
People on the Autism spectrum
Another group which is disproportionately likely to be labelled transgender is people on the autistic spectrum.(5) An article in Forbes reported that:
The potential link between ASD and gender dysphoria was noted by researchers as early as 1981...at least nine larger-scale studies have been published in the medical and psychological literature, spanning several Western countries... Across all of these studies, almost without exception, rates of ASD or autism traits range from 5% to 54% among those with gender dysphoria, significantly higher than among the general population. (6)One group of researchers, remarking on the possible driving force behind this, suggested that In our sample, 26% of the adolescent SR [Sex Reassignment] applicants were diagnosed to be on the autism spectrum... Our clinical impression is that a long-standing feeling of being different and an outsider among peers could play a role in ASD children developing gender dysphoria in adolescence. (7)
Professor Gillberg, an expert in Autism, in evidence submitted to the recent Bell versus Tavistock Judicial Review which took place last year (2020), noted the sudden growth of children on the autism spectrum with gender confusion: in 45 years of treating autistic children, he saw few cases of gender confusion until 2013. Since then there had been a worldwide explosion in the number of children saying they wanted to change sex. (8)
A documentary was broadcast a few years ago on Channel 4, followed a few children who were being seen at the Tavistock and Portman NHS Gender Identity Development Service. In this documentary you get an upclose view of one child who is on the autism spectrum and being seen as this clinic. I found it quite disturbing that they would consider putting her on puberty blockers. She has trouble communicating. She identified as a boy outside the home and girl inside the home, i.e. their identity is not fixed. At one point, one of the clinicians sensibly says it's very unclear whether Matilda particularly wants to assume a transition. The child in a way is sort of a bit unclear where they are in the world. but in spite of this the clinic seemed to push the mother a bit to put the child on puberty blockers. The mother came across as sensible and cautious about puberty blockers (i.e. chemical castration). This documentary can be viewed here: https://www.channel4.com/programmes/kids-on-the-edge/on-demand/59713-001
Outrageous Claims
Outrageously, GIRES [Gender
Identity Research and Education Society] suggested: Anecdotally, young
people who have been successfully treated, are often described as having
no residual ASD. The symptoms have disappeared once the dysphoria has been
treated.(9)
An article in The Australian
mentions a similar claim by a doctor from the US. The high-profile US
gender physician Johanna Olson-Kennedy, cited by Dr Telfer as an authority
on the mental health benefits of top surgery, has claimed there are cases
where symptoms of autism go away when (patients) are affirmed in their
(self-identified) gender. (10)
Young people with eating disorders
Another vulnerable group can be young people with eating disorders. In some cases at least, eating disorders may develop due to the stress brought on by puberty, and the fear of growing up (in girls this might be partly due to sexual harassment experienced at this age, and the growing awareness of the sexual objectification of girls and women). This group might be particularly attracted to the idea of puberty blockers. In some cases wanting to transition might be out of desperation to find something to make them feel better about their bodies.
One former patient of a gender clinic in Sweden, Johanna Berling, who also had Anorexia Nervosa, explains what the attraction was for her. I hoped Id feel good in my body. I hoped it wouldnt be a struggle to feel good in my body. That the mastectomy would make me like my body. That testosterone would make me enjoy living in my body (11)
Another young women in Britain, Ruby, who formerly identified as a boy/man and who also had an eating disorder mentions how None of the therapists that I spoke to brought that up, they didnt think that it was linked . The interviewer asks Do you? to which she replies I think so yes, because they're both...based in how I feel about my body, so, I've seen similarities between the two (12)
Children who are bullied or have had major trauma or who have psychiatric problems
Children who have experienced bullying, trauma, major life difficulties, or abuse seem to be over-represented at Gender Identity Clinics and these issues may be a factor in them developing gender dysphoria, identifying as transgender, or disassociating from their sex.
One study from Finland found that
57% ...had been significantly bullied at school...Of those who had been victims of bullying, 73% had been bullied before they came to think about their gender identity.Similar patterns occur elsewhere. This is a slide from the Gender Identity Development Service in Britain:Seventy-five per cent...had been or were currently undergoing child and adolescent psychiatric treatment for reasons other than gender dysphoria when they sought referral to SR [sex reassignment] assessment, and two more were contacted with general adolescent psychiatric services soon after entering the SR assessment(13)
In an article published in The Times in 2017, a clinician mentions a patient who came from a violent background, where older female relatives were raped. The clinician says: This girl was very tough, a real survivor. Shed gone through so much. And she said, I cant be female because girls are fragile and weak, and I dont feel like that.(14)
Fear of parental rejection may also be an influencing factor in some cases. In a documentary following children labelled/identifying as transgender, one female child is mentioned as identifying as male after their parents separated. It is mentioned that the childs Dad thought men were better than women and had wanted a male child, and wouldn't want a girl to dress like a boy. This child is now a teenager and same-sex attracted. (15)
Clinicians Raise Concerns regarding vulnerable children at Gender Identity Clinics
In an open letter to Polly Carmichael (Director of the Gender Identity Development Service (GIDS)) a former GIDS clinical psychologist, Kirsty Entwistle, raised a concern about the vulnerability of children seen at the service. She said: There are children who have had very traumatic early experiences and early losses who are being put on the medical pathway without having explored or addressed their early adverse experiences...I...believe that there are clinicians at GIDS who are putting vulnerable children on the medical pathway when they are not receiving proper input from CAMHS and Social Care with regards to mental health problems and complex family and housing difficulties. (16)
She gave some examples:
I was ...shocked by the complexity of referrals. I read many referrals of children who have been sexually abused and many children have witnessed and/or been subjected to domestic violence.A clinician in Finland who had helped set up a gender clinic there resigned from her position due to her concerns about how the patients were being treated When I realised the complexity, and realised that healthcare professionals, despite this, are still expected to okay gender-affirming treatment, despite the lack of evidence that we actually currently have, it preyed on my conscience and I wasnt prepared to take the risk, as a doctor, of causing these patients harm (17) Angela Samfjord, Head of Child and Adolescent Psychiatry, Gothenburg.I also felt that [there] was an overrepresentation of the young people who were living in poverty. I had a young person whose family were living within such extreme financial constraints that he considered it a treat to buy a can of pop. I also had another young person who was living in a very complex and unstable arrangement who arrived to sessions in a poor state of hygiene and said that there wasnt money for hygiene products. How is it ethical to undertake a gender identity assessment with the view to a medical pathway when there are children and young people [who] do not have their most basic needs met?(16) [My emphasis]
I think these examples I've mentioned show that an affirmation-only approach, and a route straight to hormones and surgery, is potential medical malpractice. As an online letter in the British Medical Journal suggested:
Confirming disgust in natal sex or external sexual organs, especially for those with prior childhood trauma, risks medical collusion with, or reenacting of, abuse. (18)Massive increase in numbers of children seen at the clinic
Before moving on to look at the treatments on offer, it is worth looking at the phenomenon of the massive increase in young people being referred to gender identity clinics, and the reversal of the sex ratio being seen at these clinics, from majority male to majority female. These same patterns appear in many different countries and may indicate that this is being driven by social factors and not just an individual internal issue.
There has been a massive increase in children presenting to Gender Identity clinics in many countries. (19) This was a nearly unheard of phenomenon a few decades ago. (20, 21)
Due to this sudden and massive increase one clinician suggested to a reporter of The Times in Britain:
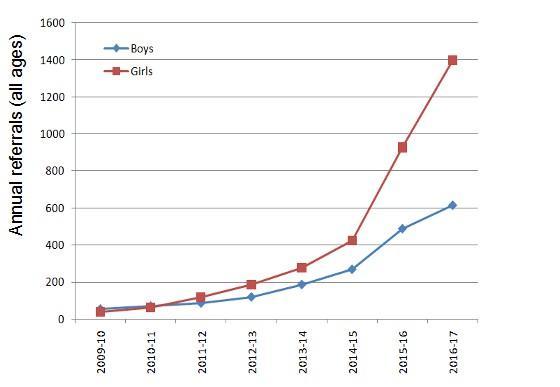
The whole service should have been halted when the number of transgender cases first exploded, one of the clinicians said. Thats the point we should have stopped because we didnt know what we were doing. (22)Just to give people an idea of the rate of increase, in Britain the Telegraph reported that:
Data shows the number of children treated at the Gender Identity Development Service (GIDS) has risen more than thirty-fold in a decade - from 77 to 2,590 (23)This graph below can help to show the increase (Source: https://www.transgendertrend.com/from-adult-males-to-teenage-girls-the-movement-from-etiology-to-ideology/)
Commenting on this increase, which is seen in many countries, a clinician, Louse Frisén, who is head of the KID team in Stockholm, Sweden that sees children with gender identity issues, said: Im just as baffled as everyone else. We dont understand why it is. Everyone in the world who works with these patients wonders the same thing (24)
Reversal in the sex ratio seen at youth clinics
There has also been a reversal of the ratio of boys to girls in the younger age group presenting at clinics for children and young people with gender identity issues. (25) This same phenomenon is happening across different countries and continents at the same time. (26)
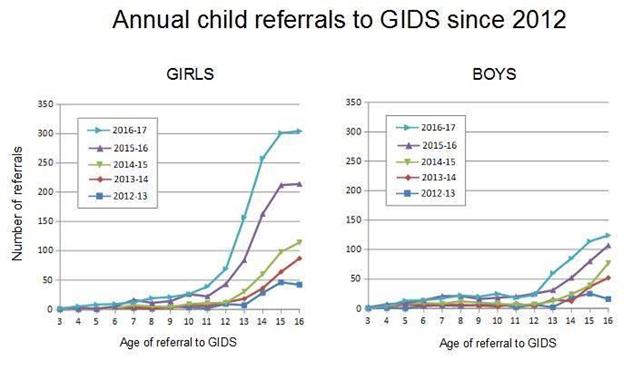
A lot of the change in pattern seems to be driven by a massive rise in teenage girls being seen at the clinics, some of whom had not previously shown signs of gender dysphoria, or who had not identified as the opposite sex when younger, but only as teens. (27)
These graphs below, looking at referrals to the Tavistocks Gender Identity Development Service in Britain, illustrate the increase in referrals, and show that the main increase is in teenage girls.
You see the same pattern in the reversal of the sex ratio elsewhere. The Canadian Gender Identity Service saw reversal of the sex ratio of patients. Between 1999 and 2005 their patients were 68% male and 32% female but between 2006 and 2013 they were 36% male and 64% female. And figures from the Dutch Center for Expertise on Gender Dysphoria show that between 1989 and 2005 referrals were 59% male and 41% female; and between 2006 and 2013 37% male and 63% female. (28)
In Ireland the numbers of minors referred to the Gender Identity Development Service are currently small, though increasing rapidly. Four times more girls than boys were referred to the Gender Identity Development Service in 2019 (34 female:8 male). (29)
Conclusion
I think these trends in children
labelled transgender are worth bearing in mind when looking at what medical
interventions are involved, which I hope to explore in the next article.
This is a new and essentially experimental area in terms of a lot of the
medical interventions. It is important to always bear in mind that Even
well intentioned medicine can do grievous harm. (30)
(2) Dr Aidan Kelly, https://www.youtube.com/watch?v=kPlCGBBcw90
(3) https://www.thetimes.co.uk/article/meet-alex-bertie-the-transgender-poster-boy-z88hgh8b8
(4) Steensma et al 2011, Desisting and persisting gender dysphoria after childhood: A qualitative study, in Clinical Child Psychology and Psychiatry https://www.acthe.fr/upload/1474384121-2011-01-07-genderdysphoria-desisting-and-persisting.pdf https://pubmed.ncbi.nlm.nih.gov/18981931/
(5)Some references on this:
https://capmh.biomedcentral.com/articles/10.1186/s13034-015-0042-y ;
Overall, 23.1% of patients
(9/39) presenting with gender dysphoria had possible, likely, or very likely
Asperger syndrome as measured by the Asperger Syndrome Diagnostic Scale
(ASDS). https://www.liebertpub.com/doi/full/10.1089/lgbt.2015.0070
;
https://link.springer.com/article/10.1007/s10803-015-2413-x
;
https://pubmed.ncbi.nlm.nih.gov/32770077/
Personal Story https://www.transgendertrend.com/autism-gender-dysphoria
About 30,000, or 5 percent,
of the cisgender people in the study have autism, the researchers found,
whereas 895, or 24 percent, of the gender-diverse people do.https://www.spectrumnews.org/news/largest-study-to-date-confirms-overlap-between-autism-and-gender-diversity/
Clinician seeing Irish patients
mentions this issue https://www.youtube.com/watch?v=kPlCGBBcw90
(7) https://capmh.biomedcentral.com/articles/10.1186/s13034-015-0042-y
(9) NHS STANDARD CONTRACT FOR GENDER IDENTITY DEVELOPMENT SERVICE FOR CHILDREN AND ADOLESCENTS SERVICE SPECIFICATION, GIRES Response, 19 April 2016. https://www.gires.org.uk/wp-content/uploads/2016/04/GIRES-Young-People-Response-to-Service-Spec-1.pdf This is the same group that produced the educational slide for teachers with blue and pink brains, mentioned in the first article in this series http://www.socialistdemocracy.org/RecentArticles/RecentSocialismFeminismTransgenderPoliticsPartOne.html
(11) https://www.youtube.com/watch?v=73-mLwWIgwU
(12) https://www.youtube.com/watch?v=7FRUDwDmkm0&feature=youtu.be
(13) https://capmh.biomedcentral.com/articles/10.1186/s13034-015-0042-y
(14) https://www.thetimes.co.uk/article/meet-alex-bertie-the-transgender-poster-boy-z88hgh8b8
(15) https://www.youtube.com/watch?v=kKMn4CymFTs&feature=youtu.be
(17) https://www.youtube.com/watch?v=73-mLwWIgwU&t=1328s
(18) https://www.bmj.com/content/364/bmj.l245/rr-1
(19) "The number of patients
keeps increasing exponentially. In the past, we used to have only ten patients
in Helsinki and Tampere, now it's hundreds we're talking about," Aino Mattila,
senior lecturer in adult psychiatry at Tampere University Hospital said,
stressing that the trend has been evident...The trend is not specific to
Finland, but rather has been noted throughout the western world.
https://sputniknews.com/europe/201804091063360965-finland-gender-reassignment-youth/
(24) https://www.youtube.com/watch?v=73-mLwWIgwU
(25) Dr Aidan Kelly https://www.youtube.com/watch?v=kPlCGBBcw90
(26) Evidence for Altered
Sex Ratio in Clinic-Referred Adolescents with Gender Dysphoria, Aitken
et al, The Journal of Sexual Medicine, 2015
https://www.ncbi.nlm.nih.gov/pubmed/25612159
(27) Rapid Onset of Gender Dysphoria in Adolescents and Young Adults: A Descriptive Study. Lisa L. Littman MPH., Journal of Adolescent Health, 2017. https://www.jahonline.org/article/S1054-139X(16)30765-0/fulltext
(28) https://transresearch.wordpress.com/2015/09/10/evidence-for-an-altered-sex-ratio-in-clinic-referred-adolescents-with-gender-dysphoria-review/ This is the study they are referencing https://pubmed.ncbi.nlm.nih.gov/25612159/
(30) https://www.bmj.com/content/360/bmj.k1312